Viet Kieu are Vietnamese who have left Viet Nam since 1975 to live in free countries around the world. Most Viet Kieu have settled in the USA; California has the largest number of Viet Kieu and Westminster, CA can boast the highest density of Vietnamese outside of Viet Nam.
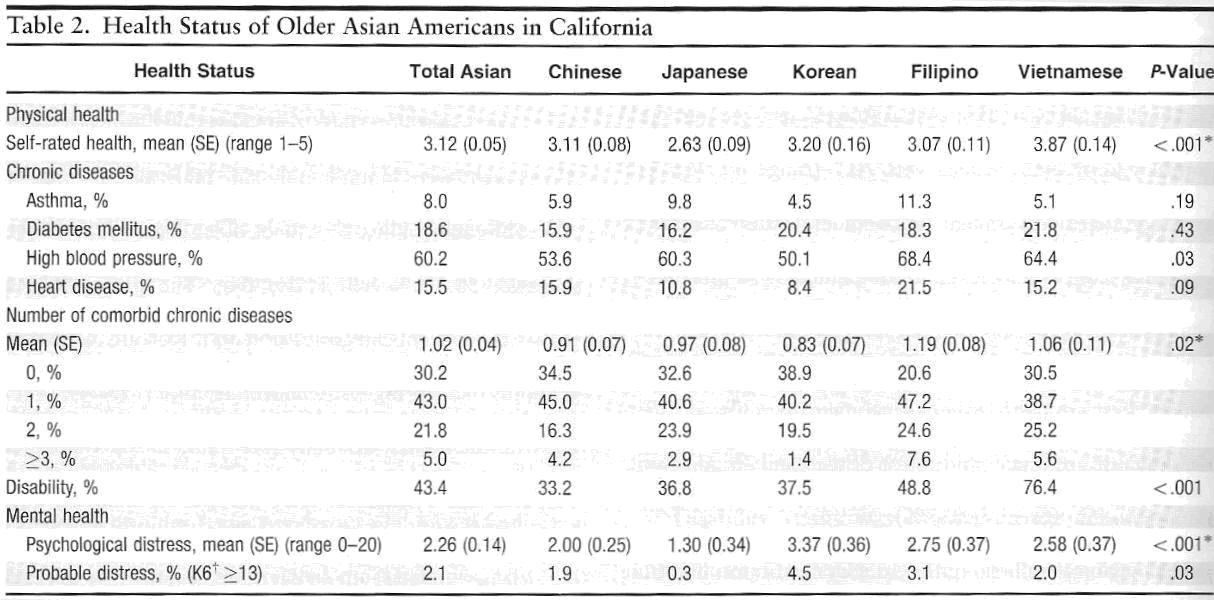
A recent paper titled “Health Status of Older Asian Americans in California”, published in the prestigious Journal of the American Geriatrics Society revealed many disturbing patterns in older Viet Kieu. Compared to other Asian-American counterparts in the “chop sticks” (Confucian) culture like Japanese-, Chinese- and Korean-Americans, older Viet Kieu, as a group are less educated, poorer , have higher rate of mental health problems, are more disabled and have the highest rate of diabetes (22%).
One can find a good explanation for most of the above findings in older Viet Kieu with the exception of higher rate of diabetes (type 2). This paper attempts to find the most likely explanation of the discrepancy and hopefully, may be able to offer some educated advice to Viet Kieu regarding Type 2 Diabetes.
What is Type 2 Diabetes?
Type 2 Diabetes is a disorder that has been misnamed, misunderstood and until 2008, the recommended treatment was completely misguided.
Unlike Type 1 Diabetes (Juvenile Diabetes) which is the only true diabetes mellitus where the lack of Insulin production from the pancreas hinders the body ability to regulate glucose by turning it to glycogen for storage therefore plasma glucose is elevated . Patients with Type 1 Diabetes have to take Insulin injections to keep their serum glucose as normal as possible. Many wears an Insulin pump programmed to mimic the pancreas release of Insulin in response to meals consumption.
It’s not that simple with Type 2 Diabetes because the elevation of glucose is caused by tissues’ resistance to the action of Insulin. The pancreas reacts to this by pumping out more and more Insulin to override the resistance; the result is Hyperinsulinemia even in fasting state.
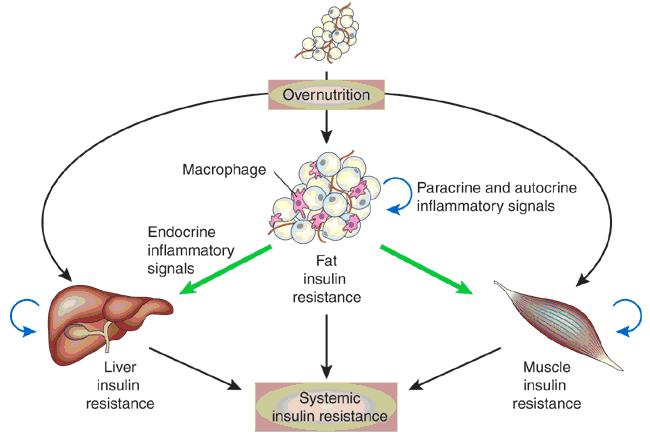
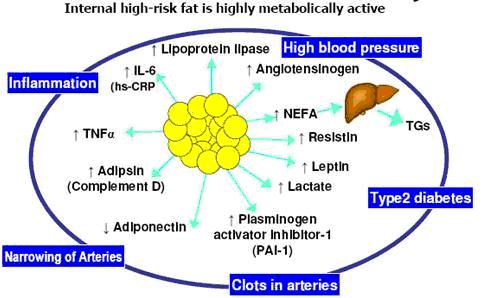
Resistance to Insulin most likely is caused by fat infiltration into various organs and the inflammatory reaction to it. This cascade of inflammation and the dysfunction of adipocytes (fat cells) which are far more active organelles than previously believed with many adipokines, adipo-related hormones , other cytokines and inflammatory reactants cause hyperlipidemia, hypertension, hyperglycemia resulting in many end organ damages i.e. cardio-vascular diseases (strokes and heart attacks), nephropathy, retinopathy, peripheral neuropathy and Alzheimer’s dementia. Of note, Insulin itself has been recognized as a pro-inflammatory reactant.
Clearly, Type 2 Diabetes is not just about high sugar (glucose) but more about hyperinsulinemia, inflammation and adipocyte dysfunction. I prefer to call it “Insulin Resistant Syndrome”, others have coined the terms Metabolic Syndrome and Syndrome X.
How treatment of Type 2 diabetes was so misguided prior to the ACCORD trial.
ACCORD (Action to Control Cardiovascular Risk in Diabetes) study is a major, well designed, multi-center study of patients with Type 2 Diabetes; sponsored by the National Institutes of Health (NIH) which started enrolling patients around 2005 and today has yielded some major findings;
1- Tight control of serum glucose using intensive Insulin regimen significantly increase mortality on those patients who, to the surprise of investigators, died from heart attacks and strokes and not by hypoglycemic reactions as suspected. This branch of the study was prematurely terminated in 2008 due to concern for the safety of the remaining study subjects.
2- As previously proven, it’s beneficial to control hypertension particularly using an ACE Inhibitor. However, lower systolic pressure to below 140 mmHg offers no extra benefit for hypertensive subjects (and might even be harmful for old people).
3- It’s important to control serum lipids using a statin drug. Adding fibrates to further lowering lipid parameters is not helpful for better clinical outcome.
Prior to this landmark study, physicians were fanatical about controlling hyperglycemia in patients with Type 2 Diabetes and treated the same way as Type 1 Diabetes. Insulin was often used when oral medications failed to achieve a fasting glucose of 110 mg% or less or when Glycosylated Hemoglobin (HGb A1C) got higher than 7. The extra Insulin given to patients who were already hyperinsulinemic wreaked havoc on their bodies and no doubt lead to premature poor outcomes as demonstrated in the ACCORD trial.
The ACCORD study should be reviewed by all current practicing physicians and should also be incorporated in the next Medicine textbooks.
A comprehensive approach to management of Insulin Resistant Syndrome should include the following:
a- There should be a sensible daily intake of limited calories ( for men between 1700 to 2000 Kcalories, for women 1500 to 1800 Kcalories per day). A Mediterranean type diet is recommended for it anti-inflammatory effect from using predominantly mono-unsaturated fat (i.e. olive oil), rich in omega-3-fatty acid from seafood and low in simple sugar (mono and disaccharides). Daily intake of protein should be at least 1.2 grams per kilogram of body weight. Only complex carbohydrates are recommended.
b- A short, 15-30 minute daily exercise program which should include aerobic and callisthenic exercises for cardio-vascular and brain fitness and some weight resistant training is recommended to maintain muscle mass to counter the effects of Insulin resistance.
c- Good management of hypertension and hyperlipidemia as mentioned earlier.
d- Stop being obsessed with glucose control. Checking fasting glucose once a day is more than enough; any level of less than 200 mg% is acceptable. Good outcomes for Type 2 Diabetes (Insulin Resistant Syndrome) are associated with HGb A1C values between 7.3-7.5, so anything less than 8 is acceptable. The only medication that has been proven beneficial in the long-term is Metformin because it makes Insulin receptors more sensitive. Other medications cost more and make the glucose readings look better but have not been shown to benefit patients; au contraire, many are downright dangerous (i.e. Insulin, Avandia etc….). Until today, the only proven beneficial effect of tight glucose control of these patients is delay of diabetic retinopathy while the risks are too many to mention.
Why are older Viet Kieu at much higher risk for Insulin Resistant Syndrome (Type 2 Diabetes) and what should be done for prevention?
Beside the comprehensive approach listed above, Viet Kieu have other problems that aggravate Insulin Resistant Syndrome and its pathology:
1- Vitamin D deficiency: this is ubiquitous in Viet Kieu living in western countries. I have yet met an older Viet Kieu with 25OH vitamin D level of greater than 34 unless he/she is taking vitamin D supplement; the reasons are many. Deficient in vitamin D (level less than 33) makes tissue more prone to the destructive effect of inflammation and aggravates Insulin resistance. All Viet Kieu should have level of 25OH vitamin D checked and take supplement if level is low. Several years ago the American Nurses Study for Osteoporosis unexpectedly showed that nurses assigned to the Vitamin D Supplement group had a 35% reduction in Type 2 Diabetes.
2- Excess consumption of Advanced Glycation End products (AGEs): AGEs can form outside or inside of the body. Inside the body, it happens when Insulin resistance causes monosaccharide to be glycolated in to AGEs compound (i.e. HGb A1C). Outside of the body, AGEs is created when food is cooked at high temperature; intentional burning of sugar (caramelize) generates large quantity of AGEs; Vietnamese cooking use this in abundant (nước kho, nước màu, nước thắng etc…). AGEs put severe oxidative stress on live tissues and have been identified as majors causes of end organ damages in Insulin Resistant Syndrome, particularly as the cause of strokes and heart attacks on patients with kidney failure. Cooking in consistently lower temperature (steam, boil) and/or adding acidic ingredients (vinegar, lemon juice, tamarind etc…) will reduce the formation of AGEs significantly.
3- Exposure to excessive amount of fructose in the environment: the USA and the rest of industrialized world have consumed less sucrose (50% fructose) and more HFCS (High Fructose Corn Syrup up to 78% fructose) in the last 20 years. Human liver can only process about 25 grams of fructose per day into energy, the rest becomes triglyceride, VLDLs free fatty acid (excess glucose is stored as glycogen) which trigger the viscera inflammatory reaction and Insulin resistance. Fructose also forms AGEs readily.
4- Lastly, although the scientific evidence is not robust, American Vietnam Veterans suffer from Type 2 Diabetes can get compensation for alleged exposure to Agent Orange during their tour of duty in Viet Nam. Could this be part of the reason for high incidence of Type 2 Diabetes in older Viet Kieu as well?
Affectionately dedicated to older Viet Kieu everywhere.
Pham H Liem QYHD20